Case Source
The below case was abstracted from the July 10th, 2024 edition of Case Records of the Massachusetts General Hospital from the New England Journal of Medicine. N Engl J Med 2024;391:167-176
Patient Presentation
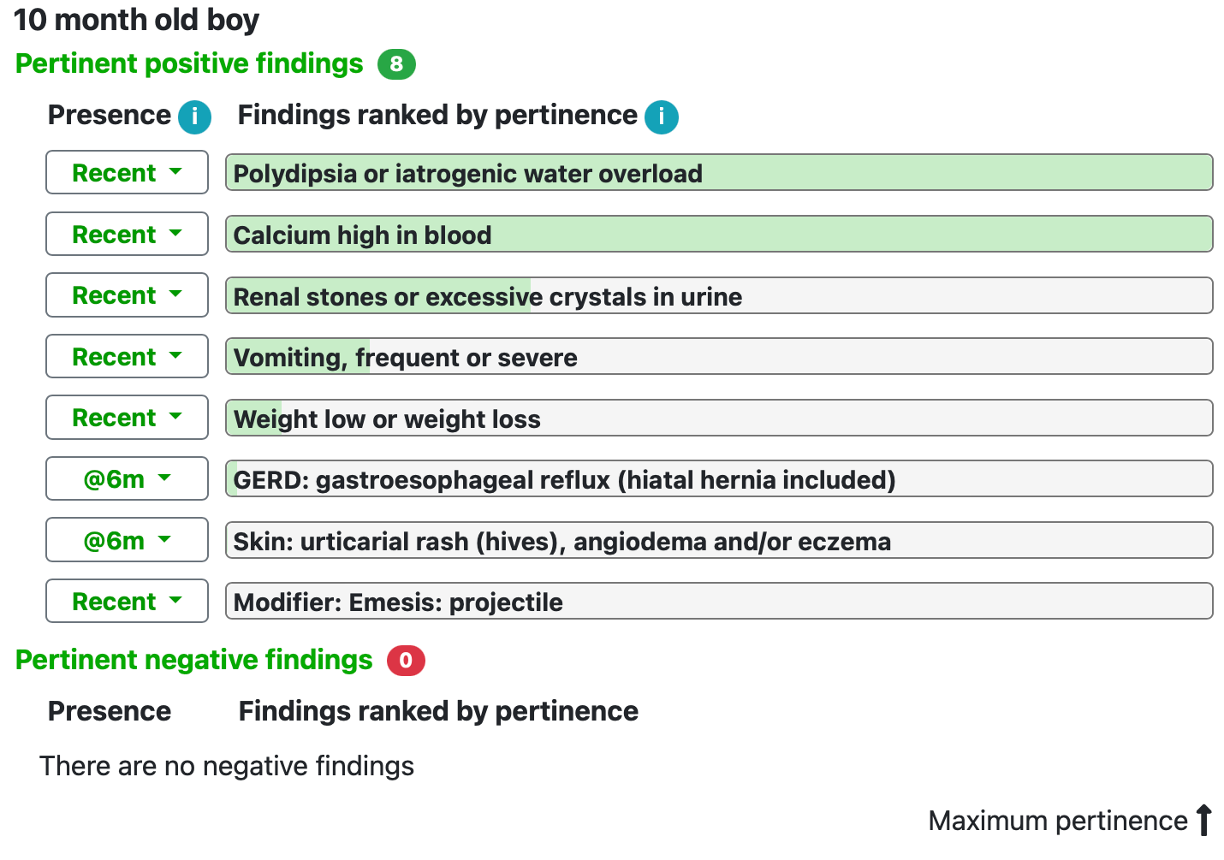
A 10-month old male patient presented to the hospital with vomiting, increased thirst and failure to thrive. He had been previously healthy until 2-weeks prior to presentation. He had been diagnosed with gastro-esophageal reflux (GERD) and eczema at an earlier outpatient evaluation. He was found to have an abnormally elevated serum calcium level. A gastrointestinal functional evaluation was unremarkable and X-rays of the knees and wrists were normal. There was evidence of bilateral medullary nephrocalcinosis.
Below is a graphical demonstration of the key presenting findings that were input in the SimulConsult software.
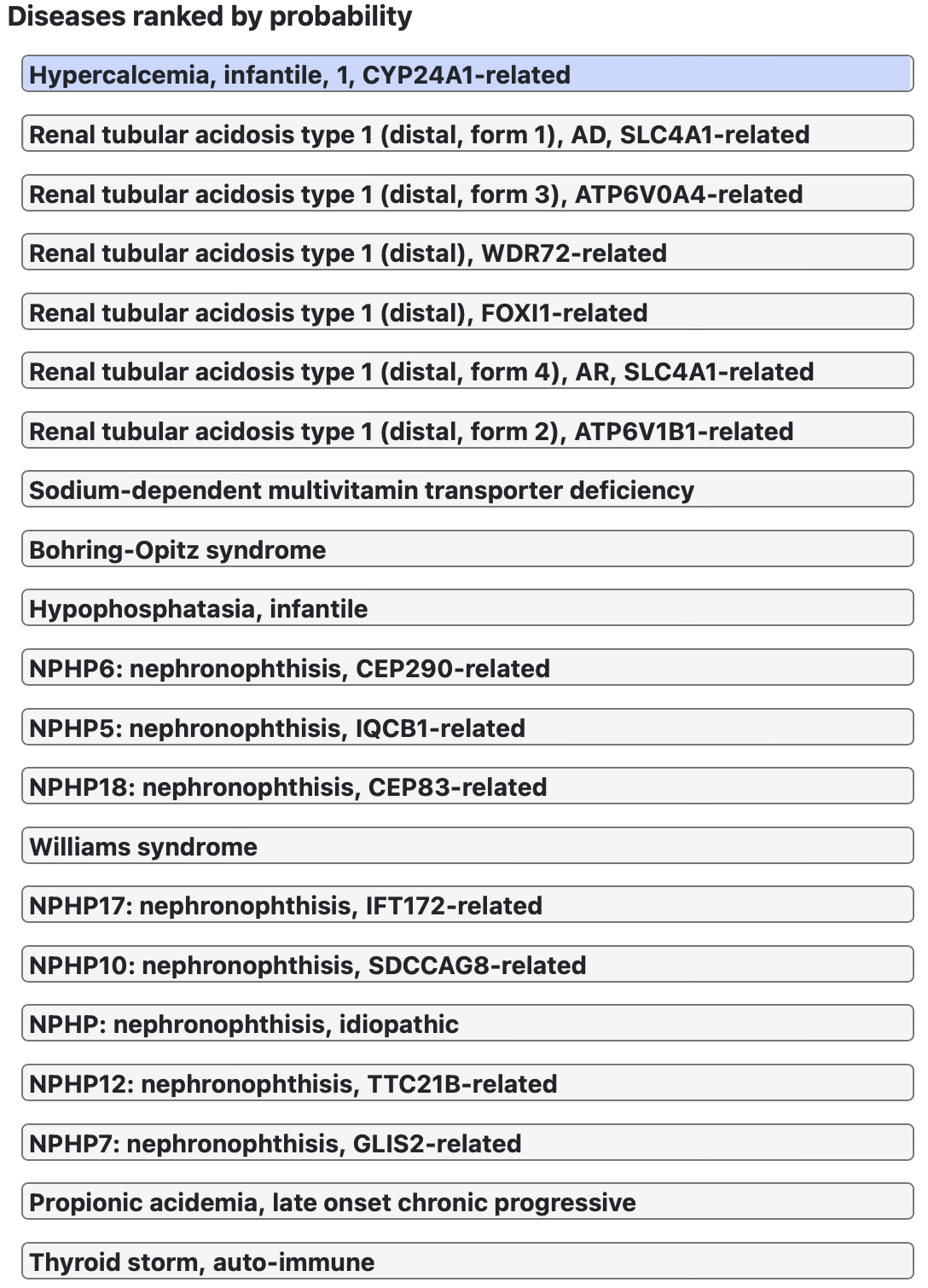
Initial SimulConsult Differential Diagnosis:
With the above findings, SimulConsult immediately identified a number of inherited disorders of calcium and vitamin D handling, renal abnormalities, Williams Syndrome and hypophosphatasia.
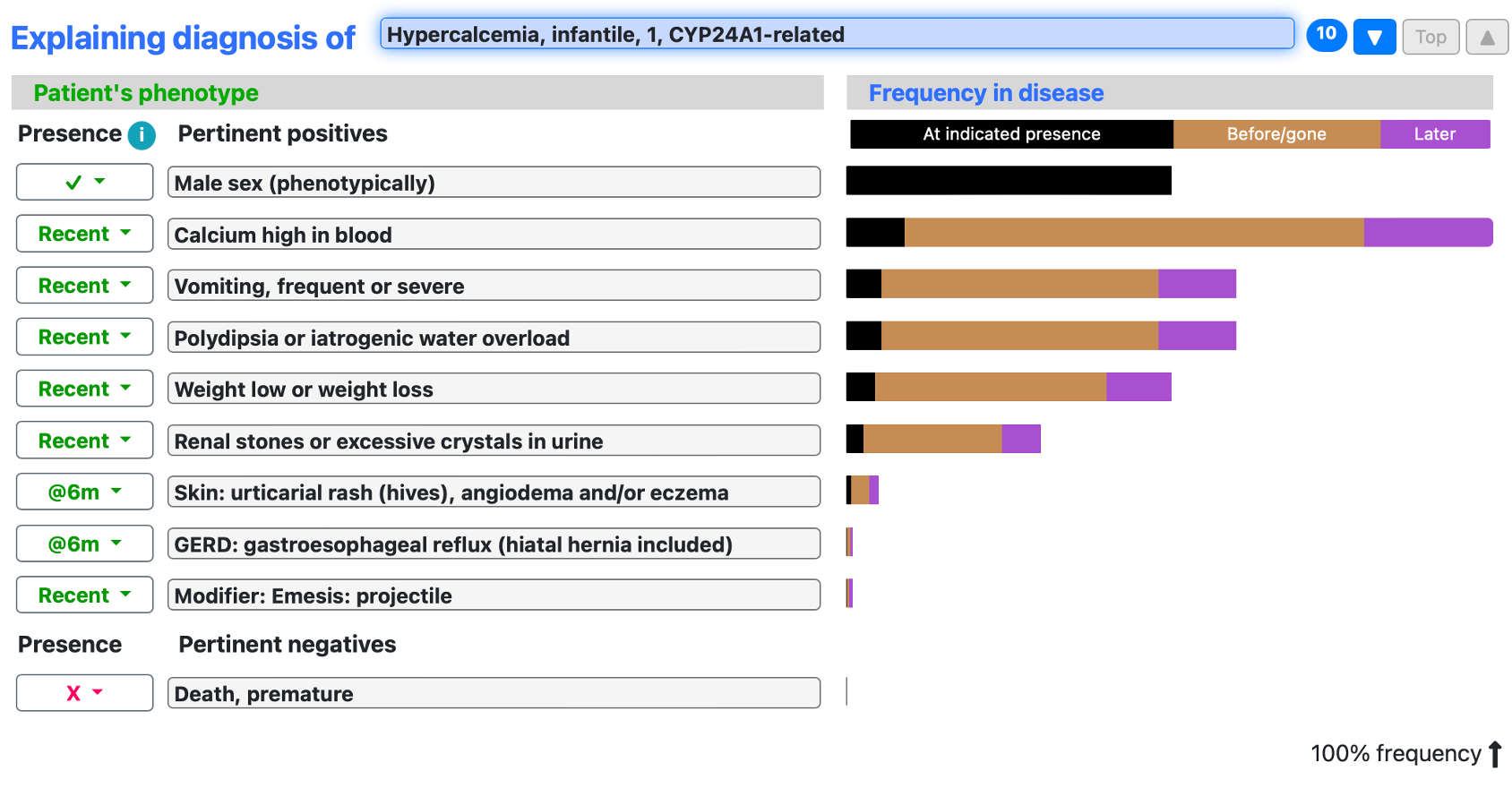
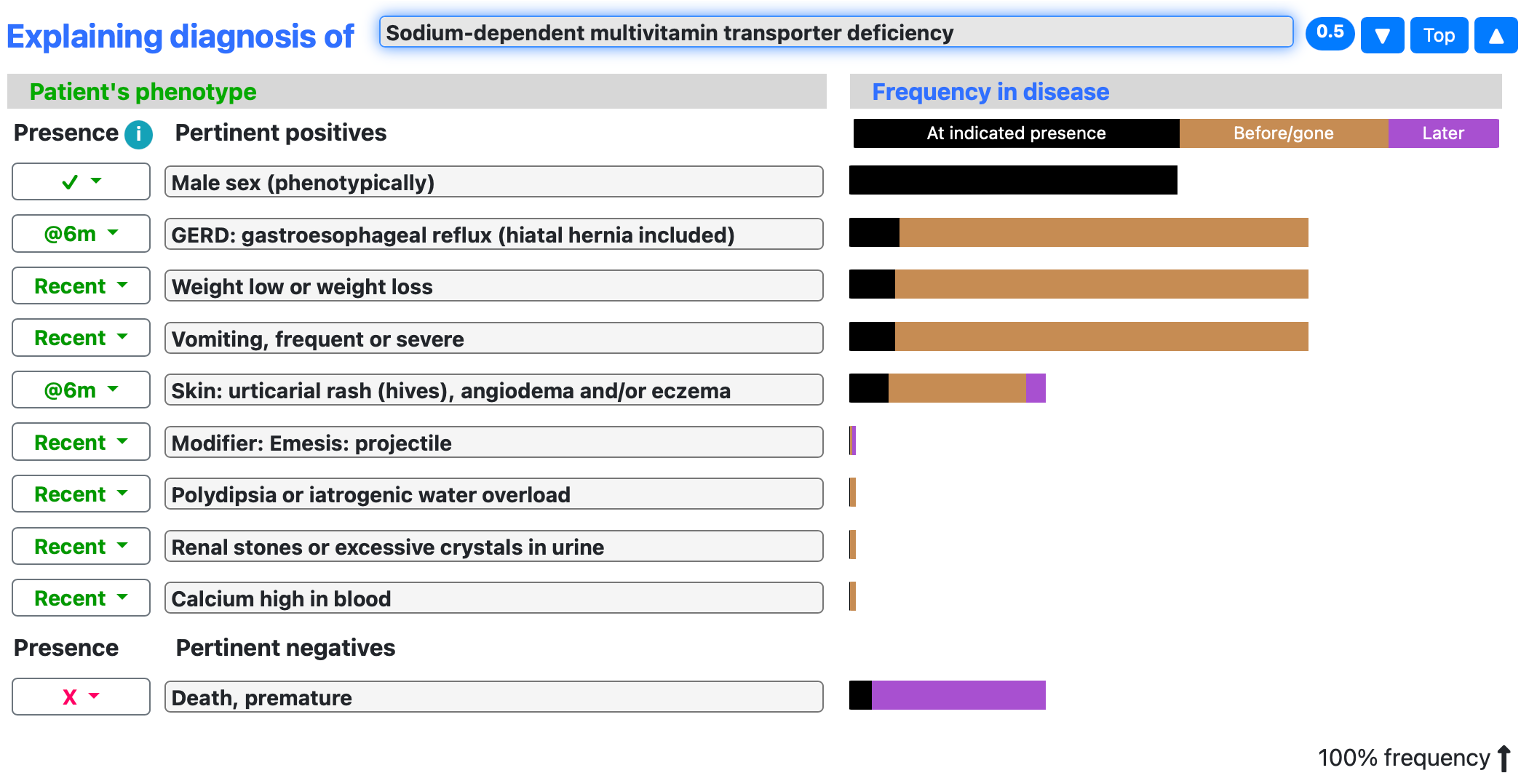
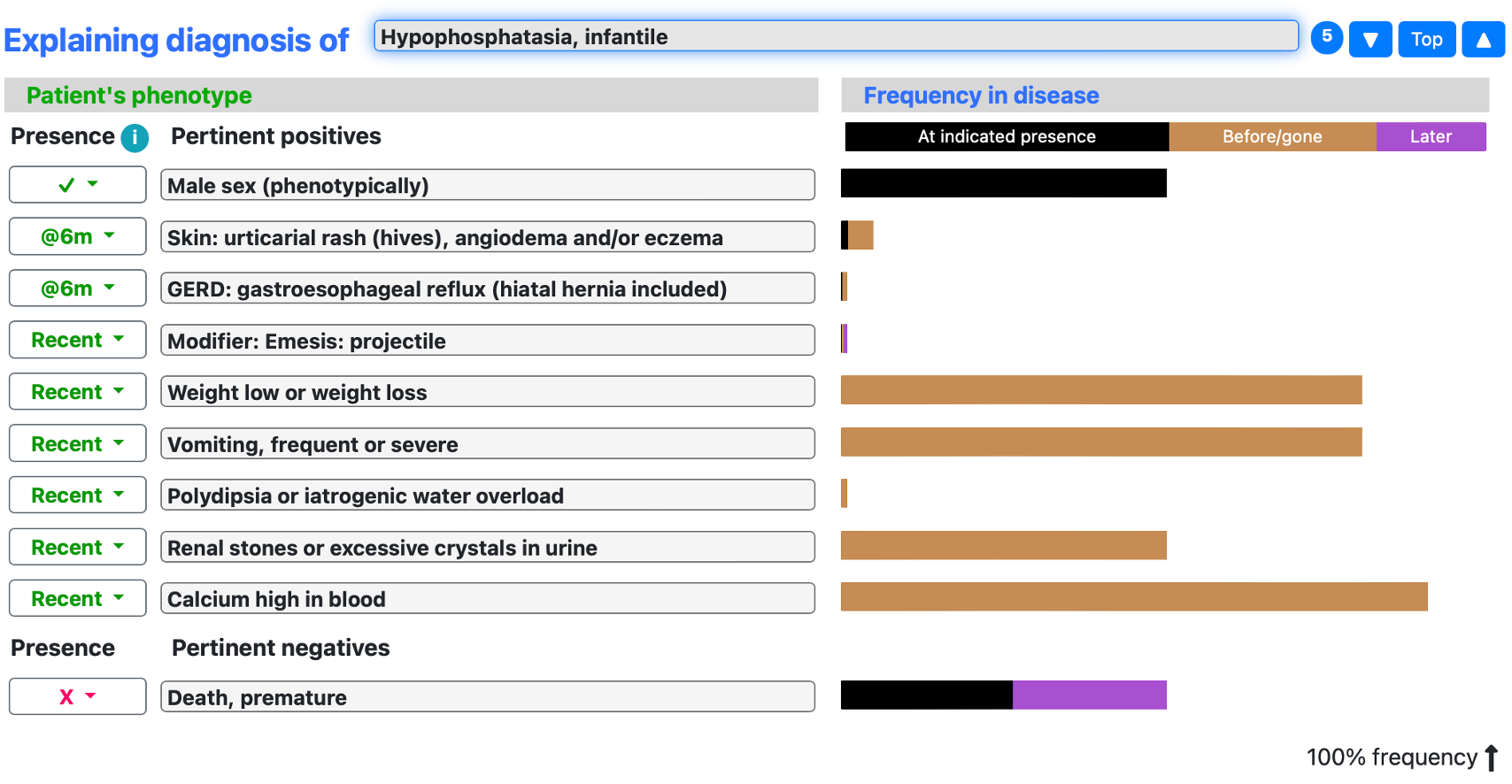
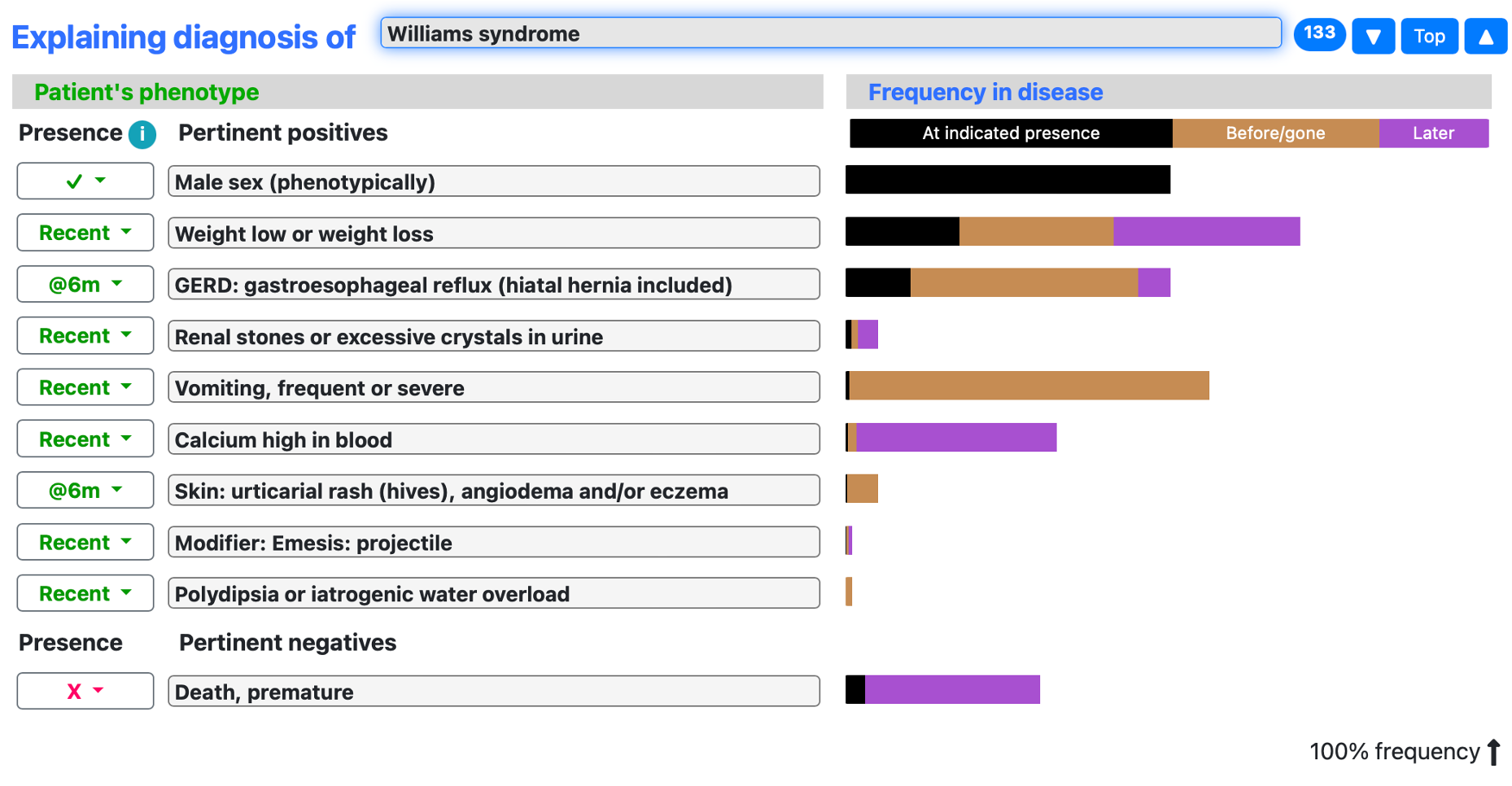
Visual explanation of the top differential diagnosis
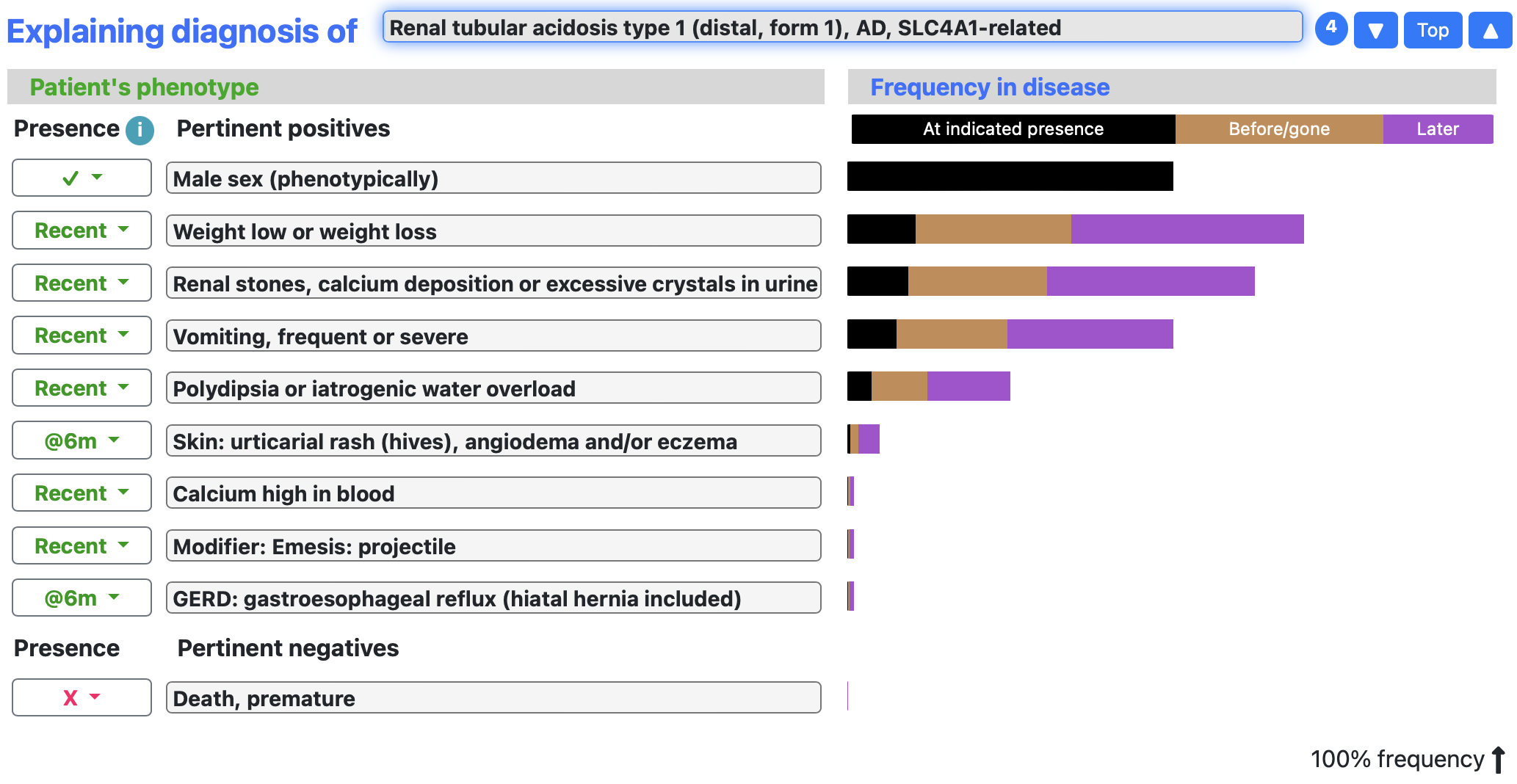
SimulConsult provides a visual explanation of the key findings that inform the differential diagnosis. This can be sorted by disease such that the viewer learns more about the selected disease and see how various findings fit within the disease state. The length of the bar illustrates the expected frequency of the selected finding and is color coded to identify findings that occur before, during or after the acute presentation of illness. Below we show a few of the top diseases identified by SimulConsult for this patient’s presentation.
Comparison between expert commentary differential diagnosis and SimulConsult differential diagnosis
The expert commentators mention a number of inherited or acquired endocrinopathies which are unlikely in this patient due to his age and normal PTH, bone imaging and history of normal development until the acute presentation of symptoms. SimulConsult included inherited renal tubular acidosis and a multivitamin transporter deficiency in the differential diagnosis as a result of weight loss, vomiting but these conditions do not routinely present with hypercalcemia and were not mentioned in the expert commentary. Similar to the assessment of the expert commentators, SimulConsult identified Williams Syndrome and infantile hyperphosphatasia. Simulconsult was in concordance with the expert opinion in ranking infantile hypercalcemia (due to CYP24A1 variant) at the top of the differential diagnosis.
Additional Diagnostic Tests
SimulConsult provides recommendations for additional testing to help narrow the differential diagnosis. The SimulConsult algorithm constantly updates these recommendations as additional findings are added. The usefulness of additional tests is ranked by SimulConsult based on the discriminative ability of additional findings to narrow the differential diagnosis. It also includes factors such as the treatability of the diagnoses and the cost of testing. Based on the findings input for the current patient SimulConsult provided the following recommendation:

By confirming that metabolic acidosis was absent, renal tubular acidosis drops substantially in the differential diagnosis.
After evaluating for metabolic acidosis, the next diagnostic step was genetic evaluation for CYP24A1 variants according to both the expert commentators and SimulConsult. The patient tested positive for abnormal CYP24A1 variants which established the diagnosis.
For users of SimulConsult, click the following link to load the patient profile and see for yourself how additional findings and tests can change the differential diagnosis.
There are more clinical cases here.