For a primary care clinician, a good rule of thumb is to focus on common conditions. By the time a patient gets to a specialist (secondary care) or to a sub-specialist (tertiary care), many common conditions have been ruled out and it is appropriate to focus more on what is a good match to a known disease and less on what diseases are common.
Accordingly, in the process of diagnosis it is appropriate to take into account the care setting because the prior probability of unusual diseases is very different in these different settings.
Example to work through
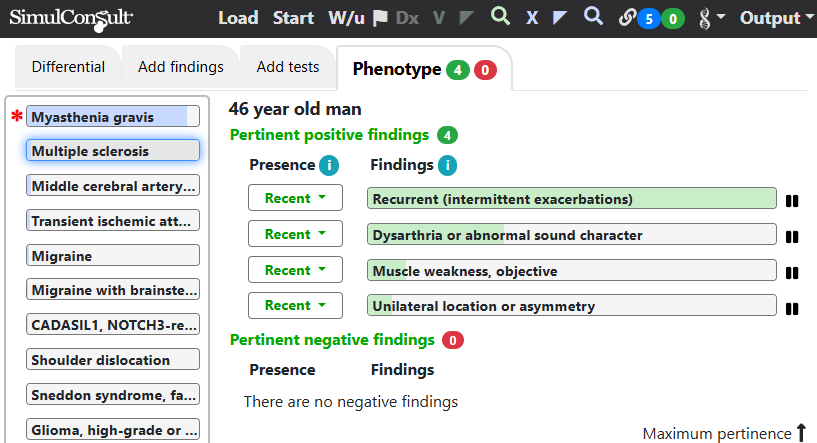
A good example comes from a case in the New England Journal of Medicine, in which a 46-year-old man had recurrent episodes of hemiparesis (weakness or the inability to move on one side of the body) and dysarthria (abnormally articulated speech). A general practitioner would think of common diseases such as multiple sclerosis and strokes. The care setting of primary care (set on the Start screen) takes this approach:
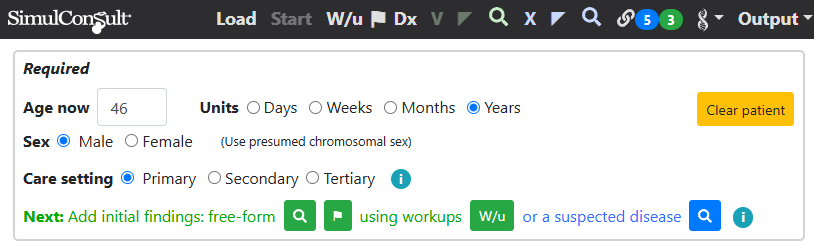
Using the findings in this case one gets a differential diagnosis focusing on common conditions, as did the clinicians in this case, who focused on multiple sclerosis: (Registered users can click the images below to jump into the software; some videos may be helpful in navigating from there)
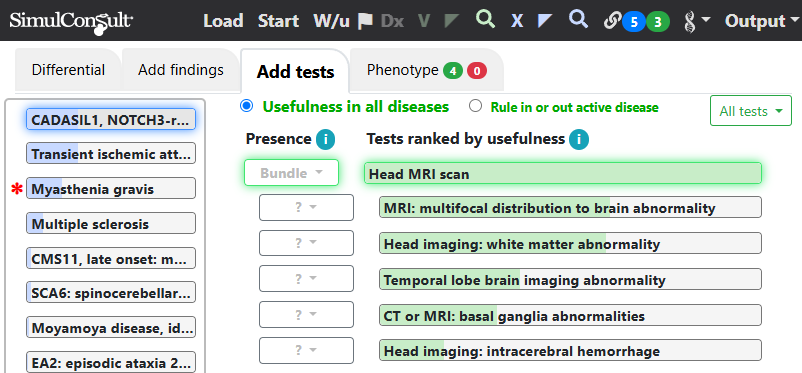
Choosing instead the tertiary care setting on the Start screen, one is prompted to consider CADASIL, which turned out to be the diagnosis, as determined on the fifth opinion by clinicians at Massachusetts General Hospital. An MRI was done that demonstrated the white matter and basal ganglia abnormalities, which were suggested as useful on the Add Tests tab of the software, as shown in the image below (in the software, clicking “Bundle” to the left of “Head MRI scan” shows the findings in the bundle).
The cognitive error associated failure to consider the care level is called “Availability”: probability of diseases assigned by vividness of memory.
This page is part of a series on the Elements of Diagnosis.
Copyright © 2025 SimulConsult