A 1 November 2009 New York Times Magazine Diagnosis column “Perplexing Pain” by Lisa Sanders MD describes a 46 year old woman with a 23 year history of “attacks of abdominal pain and fever that lasted sometimes for weeks … None of her doctors had been able to figure out what was causing the strange episodes of devastating illness” that led to a variety of exploratory surgeries and resections of her appendix, both ovaries and much of her colon. She also reported neurological symptoms:
She’d been losing feeling in her hands and feet for the past couple of years. It started off as a tingling sensation that came and went. Now her hands and feet were always numb. She could barely hold a pen, and she often stumbled because she couldn’t really feel the ground under her feet.
She had been given “countless diagnoses — one doctor thought it was lupus; another told her it was multiple sclerosis”. She saw a neurologist, who elicited further history such as very high blood pressure and vomiting during the episodes of abdominal pain, chronic constipation and episodes of bone and joint pain.
Four years earlier, she found an internist whom she trusted, and together they tried to figure out the cause of each of the many problems she had. But she felt as if they were no closer to finding answers than they were when they started. Her internist was a kind man, she told [the neurologist], but it just seemed as if every time he’d come up with some theory about what was going on and treat that, another symptom would pop up. It was like the arcade game her children played, whack-a-mole — you get rid of one problem, but then it would pop back up, along with another and another.
The neurologist decided to do an electromyography test. But even before that, one could have concluded from the available information that the diagnosis was likely to be porphyria:
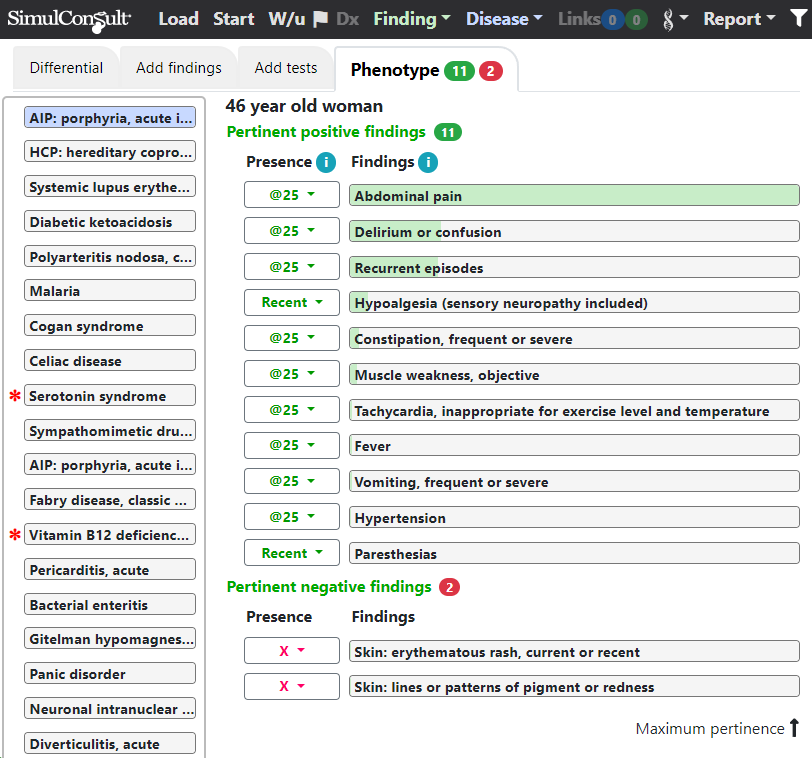
One of the problems with many diagnostic workups is that clinicians use decision trees or narrative material to look for diseases to explain one finding at a time. A key advantage of diagnostic software is the ability to help evaluate a combination of many different pertinent positive and pertinent negatives occurring at different time periods.
The red asterisks in the figure above provide risk warnings as detailed here.
Subscribers to the software can load this case by clicking on the following URL, which encodes the findings:
https://simulconsult.com/diagnose?d=16801 &u=f2&o=r11869 &u=f22&o=r11869 &u=f142&o=r11869 &u=f255&o=18261 &u=f258&o=18261 &u=f158&o=499999 &u=f0&o=499999 &u=f24&o=11869 &u=f141&o=11869 &u=f204&o=11869 &u=f239&o=11869 &u=segal_061023175759&o=11869 &u=f50&o=499999 &u=f51&o=499999 &u=f144&o=11869 &i=1 &t=c
There are more clinical cases here.